
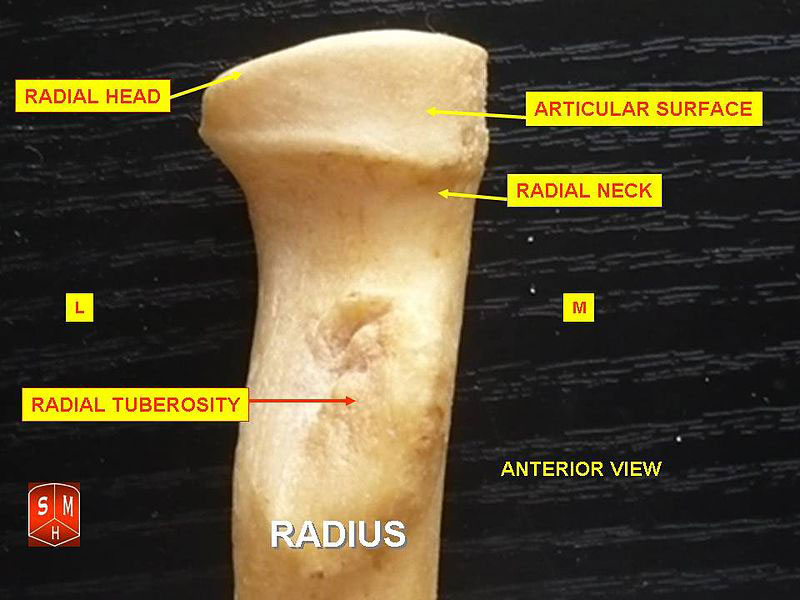
 Radial head fractures are the most common fracture in the elbow. They occur more often in women than men and in people 30-40 years old. The radial head of the elbow is a cartilage-covered rotating head located on the lateral side (outside) of the elbow. Over half of the load transfer across the elbow is through the radial head. It helps the forearm rotate palm up and palm down and to stabilize the elbow.
Radial head fractures are the most common fracture in the elbow. They occur more often in women than men and in people 30-40 years old. The radial head of the elbow is a cartilage-covered rotating head located on the lateral side (outside) of the elbow. Over half of the load transfer across the elbow is through the radial head. It helps the forearm rotate palm up and palm down and to stabilize the elbow.
 Elbows are complex joints that are like the unsung heroes of the upper extremity. They allow us to reach our mouth, head, feet and back. They contribute to palm-up and palm-down activities of daily living and motions that allow us to work and play sports. Tendons in the elbow are strong enough to withstand body weight, as in push-ups and yoga poses. Therefore, a joint that is strong and with limitless range of motion is essential to our daily lives. The elbow is a very complex joint that must be managed carefully by a specialist when an injury occurs. Loss of motion is a very common complication to any elbow injury and restoring the stability of the elbow as soon as possible is essential in order to be able to begin immediate elbow motion to prevent any further loss of motion.
Elbows are complex joints that are like the unsung heroes of the upper extremity. They allow us to reach our mouth, head, feet and back. They contribute to palm-up and palm-down activities of daily living and motions that allow us to work and play sports. Tendons in the elbow are strong enough to withstand body weight, as in push-ups and yoga poses. Therefore, a joint that is strong and with limitless range of motion is essential to our daily lives. The elbow is a very complex joint that must be managed carefully by a specialist when an injury occurs. Loss of motion is a very common complication to any elbow injury and restoring the stability of the elbow as soon as possible is essential in order to be able to begin immediate elbow motion to prevent any further loss of motion.
Cause
Radial head fractures usually occur with a fall on an outstretched hand (FOOSH) with the forearm and hand facing down (pronation) and there is an axial load across the elbow. 30% of radial head injuries have other associated injuries which can include:
- Elbow dislocation
- Medial and lateral collateral ligament MCL/LCL injuries
- Interosseous membrane disruption
- Coronoid fractures
- Terrible Triad: elbow dislocation, radial head fracture, coronoid fracture
- Carpal (wrist) fractures
- Distal radioulnar joint (DRUJ) injuries in the wrist
- Essex-Lopresti lesion: DRUJ wrist dislocation and radial head fracture
Symptoms
- Pain on the outside of the elbow
- Swelling in the elbow joint
- Pain and difficulty bending and straightening the elbow and in moving the forearm palm up and palm down
Diagnosis
Initially, a detailed history and physical exam will be performed along with x-rays. Focus should also be placed on wrist pain for associated injuries. The patient is often first seen in the Emergency Room since radial head fractures usually result from a fairly traumatic injury. Dr. Viola will order a CT Scan of the elbow to evaluate the amount of radial head fracture displacement and/or fracture comminution (fragmentation). This will determine the course of treatment depending on the fracture type:

- Type I—small, minimally displaced fracture (<2mm) with no mechanical block to rotation motion. Often these smaller fractures are not seen on plain view x-rays and therefore, CT scans are ordered. CT scan will also show the amount of displacement of the fracture and whether it is within the <2mm range.
- Type II—larger, displaced or angulated fractures >2mm with no comminution, but with mechanical block and greater loss of motion.
- Type III—multiple pieces of broken bone (comminution) which are displaced, mechanical block to motion, often significant damage to the elbow joint and ligaments stabilizing the elbow.
- Type IV—fracture and complete elbow dislocation.
If other severe associated injuries of the soft tissues of the elbow and/or wrist are suspected, as in dislocation, ligament or capsular disruption, Dr. Viola will order additional x-rays and/or an MRI to evaluate these other underlying injuries.
Dr. Viola’s Treatment Program
- Type I—non-surgical treatment. The patient can be placed in a sling or splint (absolutely no cast) for comfort for a couple of days, but then is encouraged to begin early active range of motion exercises to prevent loss of motion of the elbow and forearm. Patients are sent to Therapy to make sure they regain all of their motion. Weekly x-rays are also performed to ensure that the fracture remains non-displaced (does not shift or further worsen) while it heals over the next six weeks. Patients are allowed to slowly increase their level of activity as the fracture proves to heal without displacement.
- Type II—surgical treatment. ORIF (open reduction internal fixation) surgical treatment for the displaced fracture because it is in the joint and unstable. If joint fractures are not fixed, the fragmented incongruent bone will eventually cause cartilage wear on the joint, which leads to pain and arthritis. Fixation also allows for faster return to full range of motion and elbow use. Dr. Viola reduces the fracture openly and places screws and sometimes a plate over the fracture to stabilize the fracture and lock it together. This allows the patient to start immediate motion to prevent the elbow from becoming stiff, which is a known complication of this injury.
- Type III—surgical treatment. ORIF (open reduction internal fixation) with a plate and several screws and autologous bone graft for this more complicated, severe fracture type. One of the other known complications of the Type III radial head fracture is non-union. Dr. Viola will often use bone graft from the patient’s own (autologous) hip, leg or wrist which acts like living bone glue to fill in the fracture to ensure a better healing rate of this severe, complex fracture type. Immediate range of motion exercises are started after surgery and may be somewhat limited due to other soft tissue injuries, such as ligaments.
- Type IV—surgical fixation of the fracture with metal hardware and stabilization of the ligaments (either or both sides of the elbow) with titanium bone anchors. Immediate range of motion is started post-operatively, however it is somewhat limited due to the elbow dislocation and need to heal the ligaments stabilizing the elbow. A static brace is worn for a couple of weeks after surgery and then progression to a hinged brace for approximately 6 weeks begins so that a more aggressive arc of elbow range of motion is started and progressed, in order to prevent elbow stiffness, but yet balance the slow healing of the ligaments.
Dr. Viola is a firm proponent in restoring body parts to their original shape and function. That’s why he will always fix radial head fractures, no matter how easy or hard they are. Not fixing a displaced fracture causes future arthritic pain and loss of motion. Resecting (cutting off) the radial head can later destabilize the elbow, cause arthritis and not allow for full-use activities. Radial head resection is a common orthopedic practice for treating radial head fractures, but is can leave active patients with a less than ideal elbow for an active lifestyle. Another common practice is to replace the radial head with a metal or plastic prosthesis, as in knees and hips. But because the elbow joint is not just a weight-bearing joint like knees and hips, it must also withstand pulling forces (as in carrying), so these joint replacements don’t allow patients to return to a fully active lifestyle for the remainder of their lifetime.
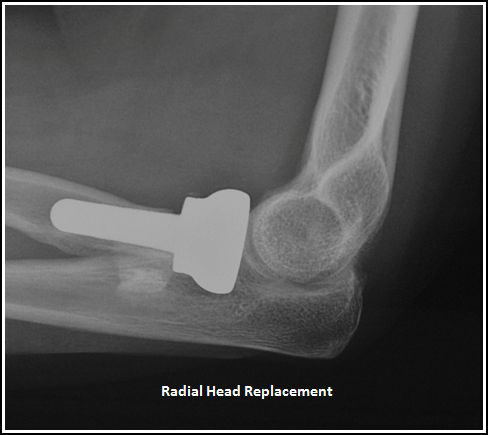 Elbow implants have come a long ways over the last few decades and can help restore painless elbow range of motion, but only allow patients to return to basic activities of daily self-care, desk work and light household activities. But the implants can also still pull, push and twist loose, become infected and even break, so they will not withstand forces for riding bikes, playing tennis, doing push ups, yoga, hammering nails, weight-lifting, etc. Thus, elbow joint replacements are reserved as a last resort for people with no remaining radial head cartilage and more sedentary lifestyles.
Elbow implants have come a long ways over the last few decades and can help restore painless elbow range of motion, but only allow patients to return to basic activities of daily self-care, desk work and light household activities. But the implants can also still pull, push and twist loose, become infected and even break, so they will not withstand forces for riding bikes, playing tennis, doing push ups, yoga, hammering nails, weight-lifting, etc. Thus, elbow joint replacements are reserved as a last resort for people with no remaining radial head cartilage and more sedentary lifestyles.
Learn How We Can Help You Stay Active