
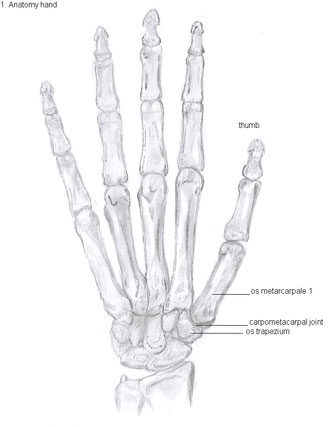
 Pain at the base of the thumb is very common. Joint pain stemming from the 1st CMC joint is one of the most common areas in the hand to develop arthritis, which is inflammation and pain resulting from cartilage loss. The 1st CMC (carpometacarpal) joint is a specialized saddle-shaped joint at the base of the thumb. The trapezium carpal bone of the wrist and the first metacarpal bone of the hand form the 1st CMC or thumb basal joint. The saddle shape of this joint, formed by the trapezium and 1st metacarpal, allows the thumb to have such a uniquely wide range of motions including up/extension, down/flexion, in/adduction, out/abduction and opposition.
Pain at the base of the thumb is very common. Joint pain stemming from the 1st CMC joint is one of the most common areas in the hand to develop arthritis, which is inflammation and pain resulting from cartilage loss. The 1st CMC (carpometacarpal) joint is a specialized saddle-shaped joint at the base of the thumb. The trapezium carpal bone of the wrist and the first metacarpal bone of the hand form the 1st CMC or thumb basal joint. The saddle shape of this joint, formed by the trapezium and 1st metacarpal, allows the thumb to have such a uniquely wide range of motions including up/extension, down/flexion, in/adduction, out/abduction and opposition.
Causes
This complex little thumb joint, for which so many people experience thumb arthritis, can break down from a number of factors. It is thought that chronic, high compressive loads, unstable joint or ligament laxity and complex range of motion are the primary contributors. Secondary contributors can include gout, rheumatoid arthritis, infection and trauma.
The 1st CMC joint allows the thumb to pivot, swivel and pinch and can take on relatively high compressive loads of energy. The joint is stabilized by the volar beak ligament on the palmar side of the hand. Over time, or with trauma, the ligament can weaken causing collapse of the basal joint. This joint, like all others, is covered with shock-absorbing cartilage. When the ligament fails to stabilize the joint, the cartilage surfaces come in direct contact with each other and eventually wear away, thus producing the all too common “bone-on-bone” scenario where there is no longer smooth, pain-free movement in the joint. Osteoarthritis (OA) is the result of this cartilage degeneration, which leads to pain, weakness, grinding and deformity.
Signs and Symptoms
Patients complain of pain in the thumb joint with a variety of activities of daily living (ADLs) including opening jars or bottles, turning door handles, turning ignition keys, buttoning shirts and pants, pinching and gripping. Weakened pinch strength, stiff thumb and swelling can also be present. Axial compression of the metacarpal upon the trapezium produces a grinding sensation that is also painful. The arthritic thumb will sometimes have a knobby deformity.
Diagnosis
 A complete history and physical exam, along with x-rays will be done initially in the clinic. X-rays show degeneration of the articular surfaces of the 1st metacarpal and trapezium, which appears as joint space narrowing, bone spurs and subluxation of the 1st metacarpal off the trapezium with a characteristic adduction stance. Dr. Viola also looks for neighboring joint arthritis, especially in the joint above the 1st CMC, which is the MP (metacarpalphalangeal) joint of the thumb and the one next to the basal joint, the STT (scaphoid-trapezium-trapezoid). It’s important to evaluate arthritis in these neighboring thumb and wrist articulations because their treatment is as equally important. Often, Dr. Viola will order an MRI to evaluate these areas because their severity affect the type of treatment done to the adjacent 1st CMC joint.
A complete history and physical exam, along with x-rays will be done initially in the clinic. X-rays show degeneration of the articular surfaces of the 1st metacarpal and trapezium, which appears as joint space narrowing, bone spurs and subluxation of the 1st metacarpal off the trapezium with a characteristic adduction stance. Dr. Viola also looks for neighboring joint arthritis, especially in the joint above the 1st CMC, which is the MP (metacarpalphalangeal) joint of the thumb and the one next to the basal joint, the STT (scaphoid-trapezium-trapezoid). It’s important to evaluate arthritis in these neighboring thumb and wrist articulations because their treatment is as equally important. Often, Dr. Viola will order an MRI to evaluate these areas because their severity affect the type of treatment done to the adjacent 1st CMC joint.
1st CMC Arthritis Treatment
Conservative treatment of thumb arthritis in early stages can be done with hand therapy, splinting, rest, activity modification and oral NSAIDs and over the counter medications for pain relief. Localized steroid injections can give temporary pain relief.
For moderate to severe arthritis, surgical treatment gives permanent pain relief and return to full activities.
 Fusion/Arthrodesis. Because Dr. Viola sees such an active patient population, his surgical treatment preference is fusion of the base of the thumb. Once the bone-on-bone arthritis is removed, so is the pain. This operation does truly restore strength and mobility and lasts longer than a joint replacement. Dr. Viola feels that active patients in their 40s, 50s, 60s and 70s are too young for a joint replacement unless there are other adjacent arthritic joints in the hand that need to be fused.
Fusion/Arthrodesis. Because Dr. Viola sees such an active patient population, his surgical treatment preference is fusion of the base of the thumb. Once the bone-on-bone arthritis is removed, so is the pain. This operation does truly restore strength and mobility and lasts longer than a joint replacement. Dr. Viola feels that active patients in their 40s, 50s, 60s and 70s are too young for a joint replacement unless there are other adjacent arthritic joints in the hand that need to be fused.
 Where many hand surgeons are hesitant to perform this operation, Dr. Viola excels at it. In fact, he has designed a system that makes this procedure easier, more efficient and successful for hand surgeons, which in turn, produces higher patient satisfaction.Dr. Viola’s fusion rates for this technique are exceptional with the use of a little bit of bone graft from the end of the radius/wrist bone and exquisitely strong titanium plate and locking variable angle screws from the Osteomed Hand Plating System.Post-operatively, range of motion of the fingers, tip of the thumb and wrist are started right away and there is allowance of light lifting and gripping until six week post-op x-rays show healing of the fusion, at which point all restrictions are lifted.
Where many hand surgeons are hesitant to perform this operation, Dr. Viola excels at it. In fact, he has designed a system that makes this procedure easier, more efficient and successful for hand surgeons, which in turn, produces higher patient satisfaction.Dr. Viola’s fusion rates for this technique are exceptional with the use of a little bit of bone graft from the end of the radius/wrist bone and exquisitely strong titanium plate and locking variable angle screws from the Osteomed Hand Plating System.Post-operatively, range of motion of the fingers, tip of the thumb and wrist are started right away and there is allowance of light lifting and gripping until six week post-op x-rays show healing of the fusion, at which point all restrictions are lifted.
Joint Replacement/Arthroplasty. Not everyone is a candidate for a fusion, so there is a role for this surgery. Even though it is called a “joint replacement” surgery, there is no actual implant unlike a knee or hip replacement, for example. The thumb moves in too many different planes that there is no device currently on the market that can accommodate the high stresses and range of motion that the thumb undergoes. Instead, Dr. Viola uses an APL to FCR tendon transfer technique to stabilize the base of the thumb after removing the arthritic trapezium articulation to the 1st metacarpal (that was causing the bone-on-bone pain). Post-operatively, patients are casted or splinted and given fairly strict use restrictions for six weeks. Motion of the fingers, tip of the thumb and forearm are allowed during this time (unlike every joint in the hand except the base of the thumb in the fusion surgery).
There are several other “joint replacement” techniques out there, but with time and extensive experience with this all-too-common problem in hand surgery, Dr. Viola has developed these solutions that seem to bring the highest patient satisfaction. The fusion allows for greater pinch strength, mobility and fusion rates with a procedure that lasts a life-time.